
The thyroid gland operates as the primary regulator of human cellular metabolism.
When physical symptoms or abnormal serological panels indicate potential endocrine dysfunction, physicians immediately mandate a comprehensive structural evaluation. Utilizing an ultrasound for thyroid diagnostics remains the global clinical gold standard for assessing the physical integrity of this highly vascularized organ.
For patients requiring precise anatomical mapping, securing a high-resolution Ultrasound Scan in Bangalore ensures the rapid, non-invasive identification of nascent pathologies.
Preventative structural screening effectively mitigates severe metabolic complications, establishing this specific radiological protocol as the Best Health Screening Test in Bangalore for proactive endocrine management.
This diagnostic modality utilizes high-frequency acoustic waves to generate exact soft-tissue maps, entirely eliminating patient exposure to ionizing radiation while providing unparalleled anatomical clarity.
Medical Disclaimer
The information provided in this clinical guide is strictly for educational purposes and does not constitute professional medical advice, diagnosis, or treatment. Always seek the direct guidance of a qualified endocrinologist, radiologist, or primary care physician regarding specific physical symptoms, diagnostic imaging requirements, and appropriate clinical protocols. Never disregard professional medical advice or delay seeking clinical evaluation based on the contents of this publication.
Key Points at a Glance
- Sub-Millimeter Resolution: Generates highly precise anatomical detail of the glandular tissue and surrounding cervical structures.
- Radiation-Free Safety: Relies strictly on acoustic wave propagation, ensuring absolute biological safety for repeated clinical surveillance and preventative monitoring.
- Real-Time Structural Visualization: Allows radiologists to dynamically evaluate physiological boundaries and internal anomalies without requiring exploratory surgical intervention.
Recognising the Clinical Triggers: Symptoms and Palpable Anomalies

Diagnostic radiological imaging is deployed exclusively when clinical evidence suggests underlying structural pathology.
When a patient presents with systemic symptoms of thyroid dysfunction, physicians must immediately transition from a generalized clinical suspicion to a precise anatomical diagnosis. Because the thyroid gland is situated deep within the anterior cervical region, manual palpation alone is insufficient for determining the cellular composition or exact dimensions of an anomaly.
Clinicians rely on a highly specific set of physiological and biochemical markers to mandate a high-resolution ultrasound referral. These triggers are broadly categorized into structural, compressive, and metabolic indicators.
Clinical Markers Mandating Radiological Intervention
The following table details the specific physical and physiological symptoms that compel an endocrinologist or primary care physician to order immediate cervical imaging:
| Clinical Marker Category | Specific Symptom or Observation | Diagnostic Rationale for Ultrasound |
|---|---|---|
| Palpable Structural Anomalies | Cervical Nodules: The physician physically detects a localized, abnormal mass in the anterior neck during a routine manual examination. | To determine the exact physical composition of the lump. The radiologist must differentiate whether the nodule is a harmless fluid-filled cyst or a dense solid mass requiring further oncological investigation. |
| Compressive Indicators | Dysphagia (Difficulty Swallowing): The patient reports a persistent sensation of physical obstruction or pressure when swallowing food or liquids. | To evaluate potential structural encroachment. An enlarged gland or a rapidly growing nodule can physically compress the adjacent esophagus, requiring imaging to measure the exact degree of airway or digestive tract obstruction. |
| Neurological Impairment | Vocal Cord Paresis (Hoarseness): Unexplained, chronic alterations in vocal pitch or severe hoarseness not associated with a standard respiratory infection. | Expansion of a malignant or large benign mass can physically impinge upon the recurrent laryngeal nerve. The scan maps the mass’s anatomical boundary relative to this critical nerve pathway. |
| Biochemical Instability | Abnormal Serological Panels: Routine blood work reveals severely elevated or depressed levels of Thyroid Stimulating Hormone (TSH), indicating Hyperthyroidism or Hypothyroidism. | To identify the structural root cause of the chemical imbalance. The ultrasound can reveal distinct glandular patterns consistent with autoimmune conditions, such as Hashimoto’s thyroiditis, which actively alter the physical texture of the tissue. |
Strictly mapping these physiological triggers to high-resolution imaging protocols, clinicians eliminate diagnostic guesswork. This rapid transition from symptom identification to structural verification allows for the immediate formulation of an accurate, highly targeted medical intervention plan.
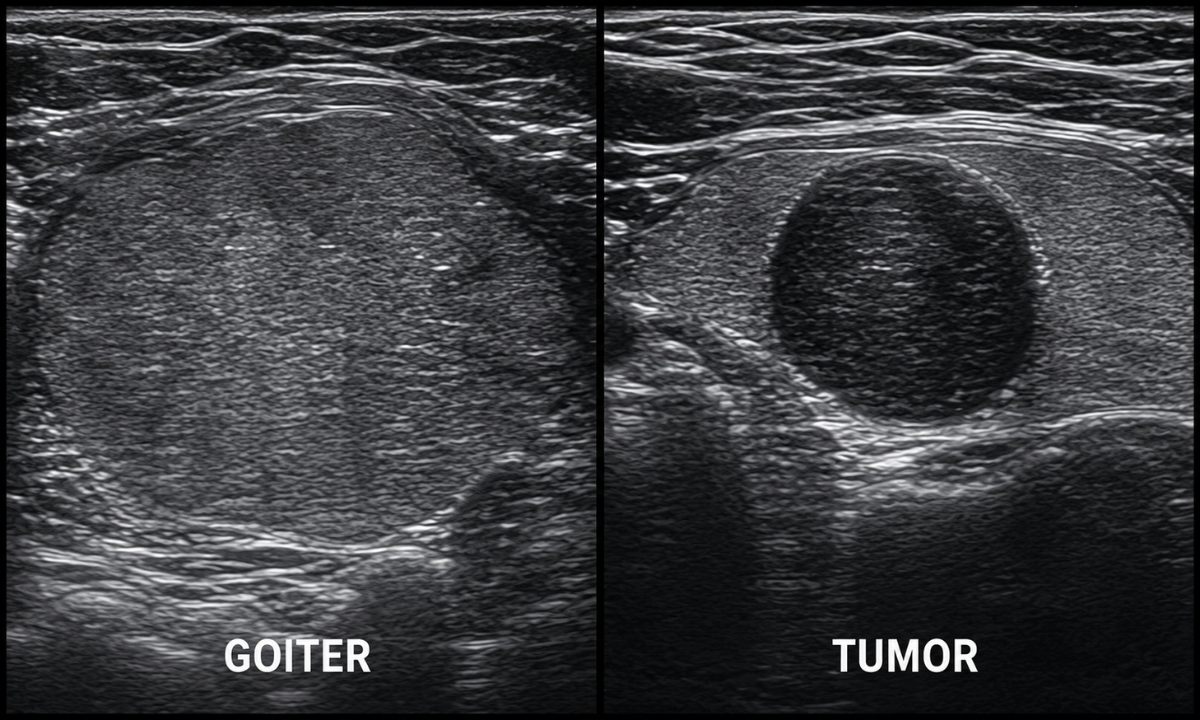
Pathomorphological Differentiation Between Goiters vs. Tumors
Once clinical triggers necessitate an imaging referral, the radiologist assumes the critical task of interpreting the structural data.
The primary objective is to differentiate between a generalized systemic response within the gland and a localized, potentially dangerous cellular mutation. High-frequency acoustic imaging provides the exact soft tissue contrast required to make this critical distinction.
The diagnostic process relies heavily on analyzing tissue density, structural margins, and localized vascularity to separate benign conditions from oncological threats.
Acoustic Profiling of Diffuse Enlargement
When a patient presents with generalized cervical swelling, the radiological assessment frequently points toward Goiter disease. This condition often results from systemic iodine deficiency or autoimmune inflammation, causing the entire gland to hypertrophy (enlarge) as it attempts to maintain metabolic equilibrium.
During the ultrasound examination, a goiter presents with highly specific sonographic signatures:
- Volumetric Expansion: The radiologist measures the physical dimensions of the right lobe, left lobe, and the central isthmus, confirming uniform bilateral enlargement that exceeds standard anatomical parameters.
- Isoechoic Tissue Density: The internal texture of the enlarged gland typically reflects sound waves similarly to the surrounding healthy strap muscles. This specific echogenicity indicates benign tissue rather than dense, aberrant cellular masses.
- Multinodular Presentation: The scan may reveal multiple distinct, fluid-filled cystic spaces distributed symmetrically throughout the tissue, which is a definitive feature of a benign multinodular goiter.
Isolating High-Risk Cellular Masses
Conversely, the identification of a solid, localized mass requires immediate oncological stratification. A single, distinct nodule exhibiting aggressive sonographic features raises the clinical suspicion of a Malignant tumor in the thyroid gland.
Radiologists utilize precise visual criteria to evaluate the biological risk profile of these isolated structures:
- Hypoechogenicity: Malignant cells pack tightly together, creating dense tissue that absorbs acoustic waves. This density causes the tumor to appear significantly darker (hypoechoic) on the clinical monitor compared to the surrounding normal glandular tissue.
- Irregular Encapsulation: Benign cysts feature smooth, distinct, and well-defined borders. Malignant tumors frequently display microlobulated or jagged margins, indicating active cellular invasion into the adjacent healthy thyroid tissue.
- Punctate Microcalcifications: The presence of tiny, bright calcium deposits within the solid mass is a primary radiological indicator of specific malignancies, notably papillary thyroid carcinoma.
- Central Angiogenesis: By activating Color Doppler technology, the radiologist evaluates the localized blood supply. While benign nodules typically demonstrate peripheral blood flow along their outer rim, malignant tumors develop chaotic central vascular networks to support rapid, unchecked cellular division.
Clinical Diagnostic Principle: The exact combination of hypoechogenicity, irregular margins, microcalcifications, and central vascularity documented during the ultrasound directly dictates the clinical necessity for a subsequent Fine Needle Aspiration (FNA) biopsy. This interventional step is required to extract cellular material for definitive pathological verification.
Why Ultrasound is the Primary Modality
While advanced imaging modalities such as Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) hold significant clinical value in systemic oncology, ultrasound remains the undisputed first-line diagnostic tool for localized cervical evaluations. The anatomical position of the thyroid gland, situated superficially just beneath the skin of the anterior neck, makes it uniquely suited for high-frequency acoustic mapping.
Physicians prioritize ultrasound over other radiological technologies due to a specific combination of engineering advantages, biological safety profiles, and dynamic imaging capabilities.
Comparative Diagnostic Efficacy
To understand the clinical preference for acoustic imaging, it is necessary to compare its operational parameters against other standard radiological tools utilized for structural assessment.
| Imaging Modality | Underlying Technology | Primary Clinical Limitation for Thyroid Evaluation | Advantage of Ultrasound |
|---|---|---|---|
| Computed Tomography (CT) | X-ray attenuation and ionizing radiation. | Exposes the patient to significant ionizing radiation. Intravenous iodine contrast used in CT scans can severely interfere with subsequent functional thyroid tests or radioactive iodine therapies. | Completely radiation-free. Does not require intravenous iodine contrast, preserving the gland’s chemical baseline for future functional testing. |
| Magnetic Resonance Imaging (MRI) | Powerful magnetic fields and radiofrequency pulses. | Exceptionally high cost, extended scan duration, and susceptibility to motion artifacts from patient breathing and swallowing during the procedure. | Rapid image acquisition. The sonographer can adjust the transducer in real-time to compensate for patient swallowing or minor movements. |
| Positron Emission Tomography (PET) | Radioactive tracer metabolism (fluorodeoxyglucose). | Lacks the microscopic anatomical resolution required to evaluate the physical margins or internal structural composition of very small nodules. | Provides sub-millimeter structural resolution, allowing for the precise measurement and categorization of nodules as small as two millimeters. |
The Eradication of Radiation Exposure
The most critical biological advantage of the thyroid ultrasound is the absolute absence of ionizing radiation. CT scans and standard X-rays utilize ionizing waves that carry sufficient energy to detach electrons from atoms, a process that can potentially damage cellular DNA over repeated exposures.
Ultrasound technology relies entirely on acoustic physics. The transducer emits high-frequency sound waves (typically between 7 to 15 Megahertz for cervical imaging) that safely propagate through the soft tissue. Because it carries zero risk of radiation-induced cellular mutation, this modality is universally approved for highly sensitive demographics, including pregnant women, pediatric patients, and individuals requiring high-frequency longitudinal monitoring of established benign nodules.
Hemodynamic Mapping via Color Doppler
Standard grayscale imaging, such as a basic CT scan, evaluates static anatomical structures. Modern ultrasound transducers are equipped with Color Doppler software, elevating the scan from a purely structural assessment to a dynamic physiological evaluation.
The Doppler effect measures the change in frequency of the sound waves as they bounce off moving targets, specifically red blood cells navigating the vascular network. This allows the radiologist to superimpose real-time hemodynamic data directly over the static anatomical image.
- Vascular Pattern Recognition: The software visually maps the precise direction and velocity of blood flow within the glandular tissue.
- Pathology Differentiation: Benign cystic structures lack internal blood flow entirely. Conversely, rapidly expanding solid masses trigger angiogenesis, creating dense, chaotic vascular networks within the center of the nodule.
- Inflammatory Assessment: Autoimmune conditions like Graves’ disease cause extreme generalized hypervascularity throughout the entire gland, creating a specific sonographic phenomenon clinically referred to as a “thyroid inferno.”
Simultaneously evaluating both microscopic tissue density and real-time blood flow, ultrasound provides the most comprehensive, immediate diagnostic profile available for anterior cervical pathologies.
Preventative Screening and High-Risk Demographics
Preventative medicine prioritizes the identification of physiological abnormalities long before clinical symptoms disrupt metabolic stability.
As early-stage thyroid nodules and subtle glandular hypertrophy frequently present without physical discomfort or visible cervical swelling, relying solely on reactive diagnostic protocols exposes patients to advanced pathological progression.
Implementing proactive acoustic imaging protocols for specific patient populations ensures early detection and significantly less invasive clinical management.
To standardize preventative care, endocrinologists stratify patients into distinct categories based on documented biological, genetic, and environmental variables.
Clinical Risk Stratification Matrix
The following matrix details the primary variables that elevate a patient’s risk profile, necessitating routine structural surveillance independent of current symptom presentation.
| Risk Category | Specific Clinical Variable | Pathological Implication |
|---|---|---|
| Biological Demographics | Female patients between the ages of thirty and sixty. | Statistically demonstrates a significantly higher incidence of autoimmune thyroiditis and asymptomatic nodular development compared to the male demographic. |
| Genetic Predisposition | First-degree relative with diagnosed thyroid carcinoma or Multiple Endocrine Neoplasia (MEN) syndromes. | Indicates a profound escalation in the probability of inherited malignant cellular mutations, requiring immediate and ongoing sonographic mapping. |
| Environmental Exposure | Documented history of ionizing radiation therapy administered to the head, neck, or upper thorax during childhood. | Represents a known, direct catalyst for cellular DNA damage, heavily correlating with the development of papillary thyroid malignancies in adulthood. |
Identifying these specific risk variables allows clinicians to establish highly targeted surveillance protocols. Routine high-frequency acoustic imaging provides a non-invasive mechanism to map the glandular architecture of these vulnerable populations at regular intervals. By establishing a structural baseline during a state of apparent thyroid health, radiologists can immediately detect microscopic morphologic changes during subsequent annual or bi-annual evaluations.
Secondary Surveillance Indicators
Beyond the primary risk matrix, clinicians also recommend prophylactic ultrasound screening for individuals presenting with specific overlapping physiological conditions:
- Patients actively managing concurrent autoimmune disorders, specifically Type 1 Diabetes Mellitus, Rheumatoid Arthritis, or Celiac Disease.
- Individuals exhibiting a chronic, unexplained elevation in systemic inflammatory markers are identified during routine serological blood panels.
- Patients undergoing long-term pharmacological treatments utilizing amiodarone or lithium, medications with known structural impacts on thyroid tissue.
Patients identified within high-risk oncological categories, specifically those with a documented familial history of medullary thyroid carcinoma, require prophylactic ultrasound screening regardless of current serological baseline stability or the absence of palpable cervical masses.
The Preventative Clinical Trajectory
Executing regular structural screenings directly alters the patient’s long-term clinical trajectory. This proactive approach ensures precise medical intervention through a distinct three-step longitudinal pathway:
- Baseline Anatomical Acquisition: Capturing the initial structural dimensions, total volume, and baseline echogenicity of the healthy gland to serve as the definitive comparative standard.
- Longitudinal Growth Tracking: Utilizing advanced imaging software to compare subsequent annual scans against the baseline, measuring the exact millimeter growth rate of any newly formed nodules.
- Preemptive Clinical Intervention: Executing an ultrasound-guided biopsy or localized tissue ablation before an aggressive malignant mass breaches the thyroid capsule or invades regional cervical lymph nodes.
Shifting the clinical focus from reactive symptom management to proactive structural mapping, high-risk demographics effectively secure their long-term metabolic stability.
Why Choose Institutional Excellence at The Koshikaa?
Executing precise radiological diagnostics requires a specialized clinical environment dedicated to high-fidelity imaging and rapid operational workflows. Koshikaa operates as a premier diagnostic facility in Bangalore, providing the specific infrastructure necessary for advanced endocrine evaluations and proactive health management.
The institution separates itself from standard screening centers by integrating advanced medical technology with highly individualized patient care protocols.
Core Operational Pillars to guarantee diagnostic excellence, Koshikaa relies on three specific institutional protocols:
| Operational Pillar | Clinical Execution at Koshikaa |
|---|---|
| Technological Superiority | The facility deploys state-of-the-art, high-frequency ultrasound systems equipped with advanced Color Doppler software. This ensures sub-millimeter soft-tissue resolution and highly accurate vascular mapping. |
| Workflow Velocity | Medical uncertainty produces unnecessary physiological stress. Koshikaa guarantees the delivery of comprehensive, radiologist-verified diagnostic reports within a strict twenty-four-hour timeframe to accelerate subsequent clinical interventions. |
| Algorithmic Personalization | The institution utilizes a proprietary health screening questionnaire before evaluation. This tool analyzes individual biological data, genetic history, and lifestyle factors to tailor the exact diagnostic pathway to the patient’s unique risk profile. |
Conclusion
Relying exclusively on physical symptoms or manual palpation to manage endocrine health exposes patients to significant pathological risks. High-resolution ultrasound provides the exact anatomical data required to detect nascent cellular mutations and glandular hypertrophy long before they escalate into complex surgical emergencies.
Patients categorized within high-risk oncological demographics, or those currently experiencing unexplained metabolic fluctuations, must prioritize structural surveillance. Schedule a comprehensive diagnostic evaluation at Koshikaa to definitively map your cervical anatomy, rule out malignant cellular activity, and actively secure your long-term metabolic stability.