
Patients experiencing acute respiratory distress frequently require immediate radiological evaluation. Securing an emergency CT scan in Bangalore or initiating a comprehensive Full-body checkup in Bangalore strictly dictates the initial medical response.
As a premier Health screening centre in Bangalore, Koshikaa recognizes that rapidly identifying a severe thoracic pathogen requires absolute diagnostic precision. Administering the correct lung infection test as well as lung infection and pneumonia immediately determines the subsequent clinical trajectory and prevents massive systemic biological failure.
According to evidence-based protocols established by the American Lung Association, delaying diagnostic intervention during an active internal infection guarantees severe cellular destruction. The multidisciplinary medical team strictly relies on precise structural imaging and targeted laboratory analysis to accurately map internal pulmonary consolidation.
To establish absolute diagnostic clarity, this comprehensive guide will detail the exact clinical presentation of severe lower respiratory events.
The subsequent sections will differentiate specific pathological classifications and outline the advanced structural imaging modalities required to optimize long-term respiratory recovery.
Clinical Presentation: Lung Infections and Symptoms

Understanding specific lung infections and symptoms strictly requires observing precise physical manifestations. When an infectious pathogen infiltrates the thoracic cavity, the biological tissue immediately initiates a massive inflammatory response. This sudden biological reaction produces highly observable physical deficits that clinically mandate immediate diagnostic testing.
To properly categorize these respiratory events, medical professionals divide the clinical presentation into specific physiological categories based entirely on the underlying biological mechanism.
Clinical Categorization of Respiratory Deficits
| Presentation Category | Pathological Mechanism | Clinical Manifestations |
|---|---|---|
| Acute Febrile Response | Systemic immune activation attempts to thermally eradicate the invading internal pathogen | Sudden high-grade fever, severe physical rigors and profound systemic diaphoresis |
| Productive Coughing | Massive bronchial secretion accumulation physically obstructs the primary airways | Violent physical expulsion of purulent biological sputum |
| Pleuritic Discomfort | Severe localized inflammation of the external pulmonary lining, known as the pleura | Acute sharp thoracic pain specifically correlating with deep structural inhalation |
| Hypoxic Distress | Massive alveolar consolidation completely prevents effective systemic oxygen exchange | Rapid shallow breathing and observable cyanosis in the peripheral extremities |
While an isolated mild fever frequently resolves without medical intervention, a combination of these severe functional deficits strictly dictates immediate emergency action. The accumulated internal fluid significantly compromises the physiological respiratory reserve.
Advanced structural radiological imaging remains the only medical methodology capable of accurately quantifying this internal biological damage before complete systemic respiratory failure occurs through advanced imaging techniques.
Pathological Differentiation of Lung Infection and Pneumonia
A lung infection represents a broad medical classification encompassing any pathogenic invasion of the respiratory tract.
Medical professionals strictly differentiate these infectious events based entirely on the exact anatomical location of the biological invasion. Differentiating a standard upper respiratory lung infection and pneumonia strictly requires evaluating the specific anatomical structures currently experiencing cellular inflammation.
To secure an accurate diagnosis, clinical pulmonologists utilize a highly specific structural classification system.
Anatomical Classification of Respiratory Infections
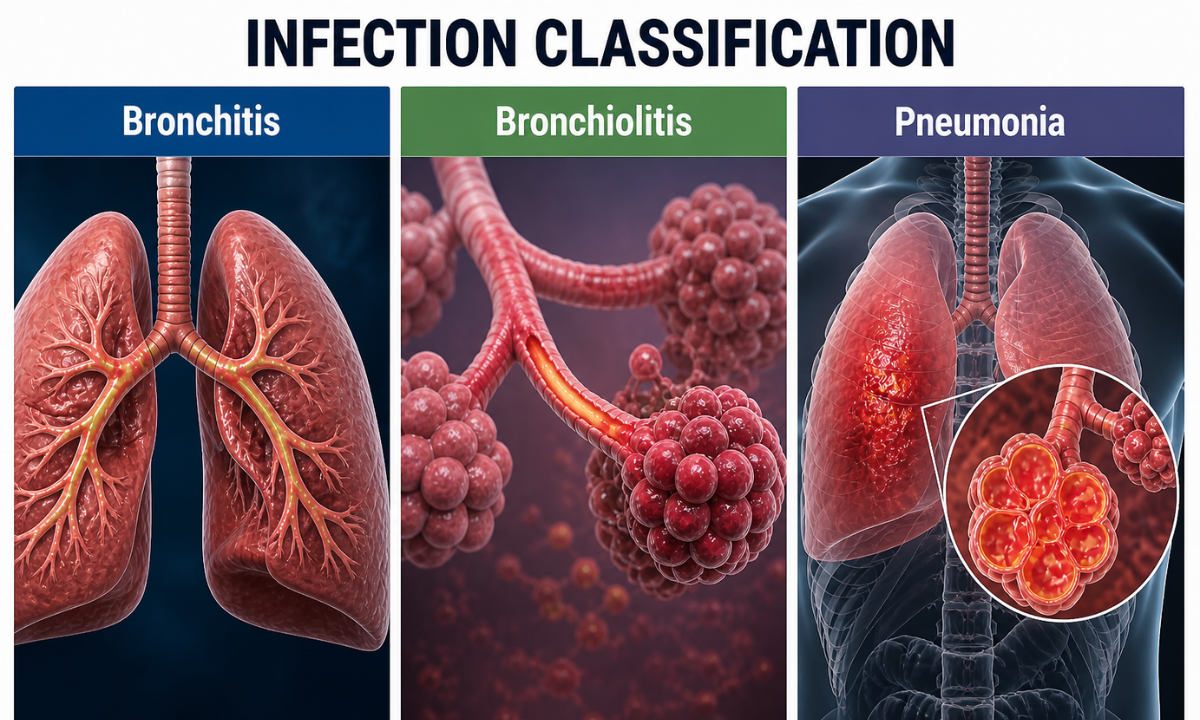
| Infection Classification | Anatomical Target | Pathological Mechanism | Clinical Severity |
|---|---|---|---|
| Bronchitis | Primary bronchial tubes | Massive mucosal inflammation of the major airway conduits, entirely without alveolar involvement | Moderate requiring standard outpatient pharmacological management |
| Bronchiolitis | Microscopic bronchioles | Severe viral inflammation strictly targeting the terminal airway passages leading to the alveoli | High risk specifically for pediatric and geriatric patient demographics |
| Pneumonia | Pulmonary alveoli | Massive pathogenic consolidation within the microscopic gas exchange sacs | Severe, requiring immediate advanced clinical intervention and radiological structural mapping |
Pneumonia represents the absolute most severe manifestation of a thoracic infection. While standard respiratory pathogens strictly target the conductive upper airways, pneumonia aggressively invades the terminal alveolar sacs.
These microscopic biological structures are directly responsible for critical systemic oxygen exchange. When a pathogen successfully breaches these structures, it triggers a highly destructive internal biological cascade.
Medical professionals monitor the following sequential physiological failures during an active alveolar infection.
- Pathogenic Infiltration: The specific bacteria or virus physically bypasses the upper respiratory immune defenses and violently invades the sterile lower pulmonary regions.
- Alveolar Engorgement: The terminal cellular sacs rapidly fill with purulent inflammatory fluid and massive amounts of dead biological cellular debris.
- Consolidation Development: The internal pathogenic fluid rapidly solidifies, creating massive, dense structural regions within the delicate pulmonary parenchyma.
- Systemic Hypoxia: The solidified purulent fluid completely blocks physiological gas exchange, physically preventing oxygen from entering the cardiovascular system.
Understanding this precise anatomical distinction is clinically vital.
Treating a generalized conductive airway infection utilizes completely different pharmacological protocols than managing severe internal alveolar consolidation.
This specific biological reality strictly necessitates definitive structural imaging to accurately differentiate the exact pathological presentation.
The Primary Evaluation Identifying Pneumonia Symptoms

When emergency medical teams evaluate severe respiratory distress, they do not immediately initiate advanced structural imaging. Identifying acute pneumonia symptoms strictly requires a comprehensive physical examination and rapid biological laboratory testing.
This initial clinical phase quantifies the exact level of systemic physiological stress and dictates the immediate pharmacological intervention required to stabilize the patient before initiating radiological protocols.
To secure an accurate initial biological baseline, clinical pulmonologists execute a highly standardized physical assessment. This hands-on evaluation allows the medical team to physically map the external manifestations of the internal thoracic infection.
Standardized Respiratory Physical Assessment
| Clinical Assessment Metric | Diagnostic Methodology | Physiological Indication |
|---|---|---|
| Pulmonary Auscultation | Utilizing a stethoscope to monitor internal respiratory acoustics | Identifying localized crackles or absent breath sounds indicates massive internal alveolar consolidation |
| Thoracic Percussion | Physically tapping the external chest wall to precisely assess internal acoustic resonance | Detecting dull acoustic responses which strictly indicate internal fluid accumulation rather than normal physiological air |
| Peripheral Pulse Oximetry | Utilizing advanced optical sensors to measure systemic arterial oxygen saturation | Quantifying the exact physical severity of the internal alveolar gas exchange failure |
| Respiratory Rate Analysis | Clinically calculating the exact number of complete respiratory cycles per minute | Identifying severe tachypnea indicates a massive physiological effort to compensate for systemic biological hypoxia |
Following this structural physical assessment, the medical team must immediately evaluate the internal biochemical environment.
Physical observations alone cannot determine the exact pathogenic cause of the biological failure. Physicians strictly require precise laboratory data to identify the specific invading organism and measure the total systemic inflammatory response.
The multidisciplinary medical team strictly mandates the following rapid biochemical evaluations.
- Complete Blood Count: This specific hematological analysis precisely quantifies the total white blood cell volume, strictly indicating the physical severity of the systemic biological immune response.
- Arterial Blood Gas Analysis: Medical professionals extract blood directly from a primary artery to definitively measure internal systemic oxygen and carbon dioxide concentrations, ensuring the internal biochemical environment remains physiologically stable.
- Sputum Culture Analysis: Clinical pathologists microscopically evaluate expelled purulent fluid to definitively identify the exact biological pathogen, allowing the medical team to administer highly targeted antimicrobial pharmacological agents.
- Systemic Inflammatory Markers: This specialized biochemical evaluation specifically quantifies a hepatic protein that the human liver produces exclusively during massive systemic internal biological inflammation.
Securing this precise physical and biochemical data provides the clinical foundation required to safely proceed.
Once the medical team mathematically quantifies the systemic biological stress, they immediately transition the patient to the radiology department for definitive cross-sectional structural mapping.
Advanced Structural Imaging: The Definitive Lung Infection Test
When preliminary physical assessments and biochemical laboratory evaluations indicate a severe lower respiratory event, physicians strictly require definitive structural visualization.
The multidisciplinary medical team must select the absolutely optimal lung infection test to accurately map the internal pathogenic consolidation. Emergency pulmonologists strictly evaluate two primary radiological modalities to secure this critical anatomical data.
Standard chest radiography frequently serves as the initial diagnostic tool; however, its physical limitations frequently obscure microscopic cellular infections.
As standard ionizing radiation passes entirely through low-density pulmonary tissue, identifying early alveolar consolidation strictly requires advanced cross-sectional imaging.
Clinical Comparison of Thoracic Imaging Modalities
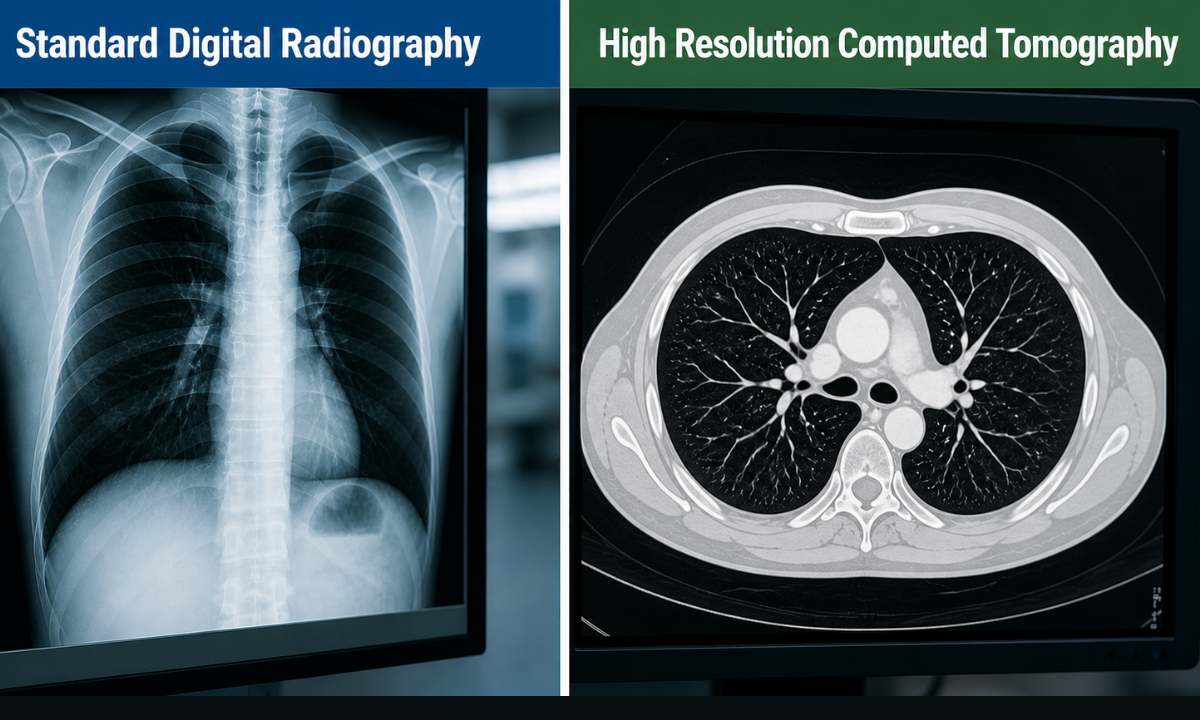
| Radiological Modality | Diagnostic Mechanism | Clinical Capability | Pathological Limitation |
|---|---|---|---|
| Standard Digital Radiography | Utilizes a single directional burst of ionizing radiation to generate a two-dimensional structural image | Rapidly identifies massive areas of internal consolidation and severe structural lung collapse | Frequently misses early microscopic alveolar infections and cannot accurately quantify deep tissue fluid accumulation |
| High Resolution Computed Tomography | Captures thousands of independent cross-sectional images from multiple precise angles | Generates a complete three-dimensional anatomical map of the entire thoracic cavity | Requires strict patient physiological stability to successfully execute the advanced scanning protocol |
To ensure absolute diagnostic accuracy during a severe respiratory crisis, medical professionals strictly prioritize computed tomography.
This precise technological capability allows clinical radiologists to definitively identify the following severe biological complications, completely invisible on a standard radiograph.
- Pleural Effusion Detection: Accurately quantifying massive purulent fluid accumulation strictly between the external pulmonary boundary and the rigid internal chest wall
- Necrotizing Pathologies: Identifying severe structural tissue death caused by highly aggressive bacterial pathogens that aggressively destroy the functional pulmonary parenchyma
- Microscopic Consolidation: Detecting millimeter-sized areas of internal alveolar fluid entirely before they merge into massive dense structural blockages
- Cavitation Formation: Precisely mapping internal structural cavities caused by chronic severe bacterial or fungal respiratory infections
Securing this advanced structural data guarantees that the medical team accurately identifies the exact physical severity of the internal biological infection.
This definitive diagnostic mapping remains the absolute foundation for initiating life-saving pharmacological interventions and targeted mechanical respiratory support.
Why Choose Koshikaa? Specialized Respiratory Diagnostics at Koshikaa
At Koshikaa, we recognize that acute respiratory infections strictly require absolute diagnostic precision. Evaluating severe pulmonary deficits demands highly advanced radiological infrastructure combined with specialized medical expertise. By choosing our diagnostic centre, patients secure direct access to several critical medical advantages.
- Rapid Acquisition Infrastructure: Our facility utilizes the latest generation of high-resolution computed tomography scanners. This ensures that every patient receives precise structural mapping in the absolute minimum amount of time.
- Specialized Thoracic Expertise: High-resolution internal data strictly requires expert medical analysis. Our dedicated team of clinical radiologists possesses the specific pulmonary expertise required to accurately identify microscopic alveolar fluid and severe necrotizing pathogens.
- Immediate Clinical Reporting: During a respiratory emergency, we completely prioritize immediate diagnostic reporting. By streamlining our internal evaluation processes, we ensure referring emergency physicians and pulmonologists receive precise radiological data instantly, allowing for immediate targeted pharmacological intervention.
Choosing Koshikaa guarantees access to a highly sophisticated diagnostic environment where clinical speed and absolute precision strictly dictate your emergency respiratory care.
Conclusion
Navigating a severe respiratory infection strictly requires an immediate evidence-based medical response. Waiting for severe physical deficits to naturally resolve guarantees massive permanent cellular destruction within the pulmonary alveoli. Rapid structural imaging utilizing advanced diagnostic technology remains the absolute foundation of early medical intervention and long-term respiratory survival.
If you observe sudden, severe respiratory deficits, seek emergency medical intervention immediately. Secure your advanced lung infection test at Koshikaa to obtain the precise diagnostic data strictly required to optimize your long-term functional recovery.