Patients experiencing the severe pelvic pain and burning sensation characteristic of a bacterial infection often visit a Health screening centre in Bangalore for immediate clinical intervention.
While a standard laboratory culture identifies the specific bacteria responsible for the immediate symptoms, recurrent or highly complex cases frequently require an advanced Ultrasound scan in Bangalore to visualize the internal pelvic anatomy.
Physicians specifically order a targeted ultrasound for uti to evaluate the structural integrity of the kidneys, ureters, and bladder, ensuring that no physical blockages or anatomical defects are causing the recurrent infections.
Because the urinary tract relies on a unidirectional flow of fluid to constantly flush out harmful bacteria, any structural abnormality can lead to severe, ascending infections that threaten long term renal function.
This comprehensive clinical guide will explore the specific diagnostic utility of sonography in managing these complex infections by addressing the following critical areas:
- The clinical threshold for radiological imaging: We will clearly define the medical difference between a simple, uncomplicated infection and a complex case that mandates immediate structural visualization.
- The specific anatomical indicators of active infection: We will detail the exact pathological changes a radiologist looks for on the monitor, including muscular wall thickening, localized inflammation, and the presence of obstructive calculi.
- The interpretation of the final diagnostic data: We will explain how the referring urologist utilizes the quantitative measurements from the final report to adjust antibiotic therapies or plan necessary surgical interventions.
After understanding these advanced diagnostic protocols, patients can better appreciate the critical role of radiological imaging in preserving long term renal health and completely eradicating chronic systemic infections.
When is Imaging Medically Necessary?
The vast majority of urinary tract infections present as uncomplicated cystitis, primarily affecting the lower urinary tract in healthy adult females.
In these standard clinical scenarios, physicians typically rely on a urinalysis and a targeted bacterial culture to prescribe an effective course of oral antibiotics. Structural imaging is not medically necessary for an isolated, uncomplicated infection.
However, when a patient presents with a complicated clinical profile or highly atypical symptoms, the immediate implementation of radiological imaging becomes a critical diagnostic requirement.
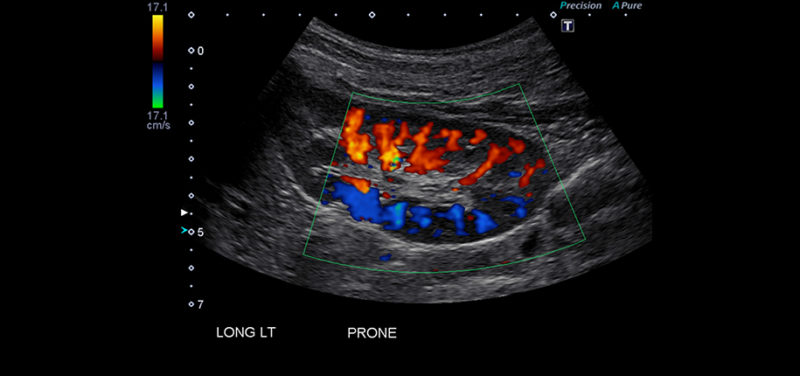
Image: Ultrasound in Diagnosing Urinary Tract Infections
A complicated urinary tract infection indicates that underlying anatomical, functional, or systemic factors are actively compromising the body’s ability to clear the bacterial pathogen. In these elevated risk scenarios, the infection can rapidly ascend from the bladder, travel upward through the ureters, and aggressively invade the renal parenchyma.
To prevent severe systemic complications such as sepsis or permanent renal scarring, referring physicians rely on ultrasound imaging to evaluate the entire retroperitoneal and pelvic space.
Urologists and primary care physicians will specifically mandate a sonographic evaluation under the following clinical circumstances:
Recurrent Infections: This is clinically defined as two or more confirmed bacterial infections within a six month period, or three or more distinct infections within a single year.
Sonography is essential to rule out chronic urinary retention, structural diverticula, or the presence of infected kidney stones that may be acting as secure biological reservoirs for the bacteria.
Acute Pyelonephritis: When a patient presents with severe unilateral flank pain, systemic chills, and a high fever, the bacterial infection has likely successfully reached the upper urinary tract.
An ultrasound is immediately ordered to detect renal abscesses, evaluate localized areas of severe tissue inflammation, and rule out any physical blockages causing infected urine to back up into the kidneys.
Gross Hematuria: The visible presence of red blood cells in the patient’s urine during an active infection warrants immediate structural evaluation.
While inflammation can cause microscopic bleeding, gross hematuria requires imaging to rule out hemorrhagic cystitis, obstructing mineral calculi, or underlying malignant growths that might be temporarily masked by the infectious process.
Atypical Patient Demographics: Because the anatomical male urethra is significantly longer than the female urethra, standard ascending bacterial infections are statistically rare in adult men.
A confirmed urinary tract infection in a male patient automatically triggers an imaging order to investigate internal structural anomalies, such as benign prostatic hyperplasia, which can cause incomplete bladder emptying and subsequent bacterial overgrowth.
Clinical Treatment Failure: If a patient shows absolutely no clinical improvement in their symptoms after seventy two hours of targeted, culture specific antibiotic therapy, an ultrasound is strictly required.
The radiologist must investigate potential anatomical blockages, such as a localized abscess or a trapped ureteral stone, which may be physically preventing the prescribed medication from successfully reaching the infected tissues.
By immediately deploying acoustic imaging in these specific scenarios, physicians can accurately identify the mechanical or structural root cause of the complicated infection and prevent irreversible damage to the urinary system.
Pediatric and Obstetric Diagnostics

When evaluating specialized patient demographics, specifically pregnant women and pediatric patients, the clinical stakes of a bacterial urinary infection are significantly elevated. For these highly vulnerable populations, standard diagnostic protocols require immediate and strict modification.
The primary medical directive is to obtain comprehensive anatomical data while completely avoiding patient exposure to the harmful ionizing radiation associated with Computed Tomography scans.
Consequently, a targeted ultrasound for uti serves as the primary diagnostic modality for structural evaluation in these specific groups. Infants and children who present with a confirmed bacterial infection of the urinary tract require immediate structural imaging.
Unlike adult patients, where urinary infections are typically acquired environmentally, pediatric infections frequently serve as the first clinical indicator of a congenital anatomical defect. The most common structural anomaly identified is Vesicoureteral Reflux.
This specific condition occurs when a defective anatomical valve allows infected urine to flow backward from the bladder up into the developing kidneys. Identifying these congenital abnormalities early through sonography is strictly necessary to initiate preventative antibiotic therapies, avoid irreversible renal scarring, and prevent long term organ failure.
Similarly, pregnant women face unique physiological challenges that significantly increase their risk for severe upper urinary tract infections.
The mechanical pressure of the expanding gravid uterus physically compresses the ureters and the bladder, while elevated maternal progesterone levels cause the smooth muscle of the urinary tract to relax and physically dilate.
This biological combination frequently causes urinary stasis, meaning urine remains trapped in the bladder, which creates an optimal biological environment for rapid bacterial proliferation. Because fetal exposure to ionizing radiation is strictly contraindicated, obstetricians rely entirely on safe acoustic imaging to monitor maternal renal health and rapidly detect complications such as acute pyelonephritis.
Diagnostic Focus in Specialized Populations
| Patient Demographic | Primary Physiological Risk Factor | Primary Sonographic Objective |
| Pediatric Patients (Infants and Children) | High prevalence of undiagnosed congenital structural anomalies of the urinary system. | To definitively identify Vesicoureteral Reflux, anatomical blockages, and congenital tissue hypoplasia without utilizing ionizing radiation. |
| Obstetric Patients (Pregnant Women) | Hormonal dilation of the ureters and mechanical compression of the bladder by the expanding uterus. | To safely identify maternal hydronephrosis, detect obstructive urinary calculi, and diagnose acute pyelonephritis without risking fetal radiation exposure. |
By prioritizing non-invasive acoustic imaging for these specific demographic groups, the interpreting radiologist provides the referring physician with the exact structural data required to treat the complex infection aggressively while maintaining absolute patient and fetal safety.
The Diagnostic Procedure and Mapping the Urinary Tract
When a referring physician orders structural imaging to investigate a complicated clinical presentation, the patient will undergo a highly specific diagnostic protocol known as a Kidney, Ureter, and Bladder (KUB) ultrasound.
A urinary tract infection ultrasound scan is a completely non-invasive, painless outpatient procedure that typically concludes within thirty to forty five minutes.
To capture the highest resolution images of the retroperitoneal and pelvic organs, the interpreting radiologist and the clinical sonographer must strictly adhere to a standardized imaging methodology.
The absolute most critical component of this diagnostic procedure occurs before the patient even enters the examination room. The facility will instruct the patient to consume a large volume of water approximately one hour prior to the scheduled scan and to strictly avoid emptying their bladder.
A fully distended urinary bladder is a physiological necessity for this specific examination. Because high frequency sound waves cannot penetrate the dense air pockets and metabolic gases naturally present within the human intestinal tract, a fluid filled bladder acts as an essential acoustic window.
The static volume of water physically displaces the overlying bowel loops, allowing the sound waves to travel uninterrupted into the deep pelvic cavity. This clear acoustic pathway is strictly required to visualize the muscular bladder walls, the insertion points of the distal ureters, and the reproductive organs located directly posterior to the bladder.
The Step by Step Sonographic Protocol
Initial Supine Imaging: The patient is positioned flat on their back on the clinical examination table. The sonographer applies a specialized, water based conductive gel to the abdominal and pelvic skin.
This gel completely eliminates any microscopic air gaps between the epidermis and the handheld transducer, guaranteeing continuous acoustic transmission.
Renal and Ureteral Evaluation: The technologist systematically sweeps the transducer across the upper bilateral flanks to evaluate the kidneys.
The sonographer measures the exact total length, width, and cortical thickness of both organs. The renal pelvis is carefully examined for any signs of physical dilation caused by trapped infected fluid. The technologist will then attempt to trace the pathway of the ureters downward toward the pelvis.
Pre Void Bladder Assessment: Utilizing the full bladder as the acoustic window, the sonographer evaluates the internal lower pelvic structures.
The technologist measures the total fluid volume currently held within the bladder and meticulously examines the mucosal lining for any localized thickening, inflammatory debris, or obstructive stones lodged at the ureterovesical junction.
Post Void Residual Measurement: Following the initial imaging sequence, the sonographer will instruct the patient to visit the restroom and completely empty their bladder. The patient then returns to the examination table for a final, critical scan.
The technologist measures any remaining urine left inside the bladder. A high post void residual volume is a primary clinical indicator of urinary retention, which frequently serves as the mechanical root cause of chronic bacterial infections.
Systematically mapping the entire urinary tract before and immediately after urination, the radiologist gathers the precise structural and functional data required to diagnose the physical anomalies driving the complicated infection.
Key Sonographic Indicators
When evaluating the retroperitoneal and pelvic cavities, the interpreting radiologist systematically analyzes the acoustic data to identify specific structural deviations. Normal, healthy urinary organs produce standard, predictable acoustic echoes.
However, when bacterial pathogens invade the tissues, the resulting inflammation, swelling, and fluid accumulation drastically alter these normal echo patterns.
Documenting these precise urinary tract infection ultrasound findings provides the referring physician with definitive evidence regarding the infection’s physical severity and precise anatomical location.
During the evaluation, the radiologist cross references the real time visual data against a standardized list of recognized clinical pathologies. The presence of any of the following structural abnormalities immediately confirms a complicated diagnosis.
Diagnostic Mapping of Sonographic Pathologies
| Clinical Pathology | Primary Sonographic Indicator | Diagnostic Implication |
|---|---|---|
Severe Cystitis | Diffuse or focal thickening of the muscular bladder wall exceeding three millimeters when the bladder is fully distended. The sonogram may also reveal mobile, echogenic debris floating within the luminal fluid. | Confirms advanced lower urinary tract inflammation, highly common in chronic, treatment resistant infections. |
Acute Pyelonephritis | Global physical enlargement of the affected kidney, a loss of the normal visual distinction between the cortex and the medulla, and localized hypoechoic (dark) regions indicating severe tissue edema. | Confirms the bacterial infection has successfully ascended from the bladder and actively invaded the functional renal tissue. |
Renal or Perirenal Abscess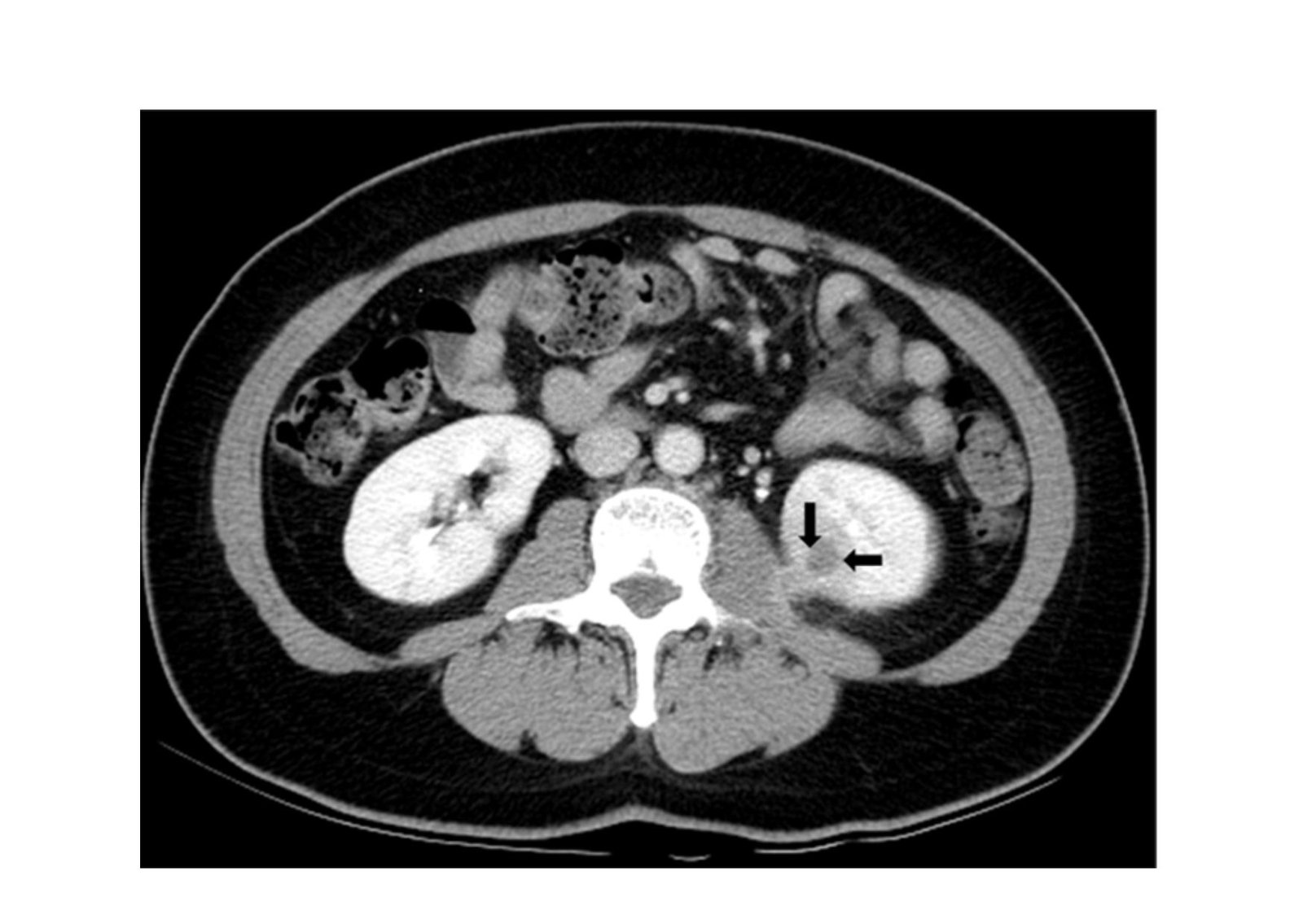 | A clearly defined, complex cystic structure featuring thick, irregular walls and internal fluid debris, often located within the renal parenchyma or the immediately adjacent fatty tissue. | Identifies a dangerous, localized collection of infected pus that typically requires immediate intravenous antibiotics or targeted surgical drainage. |
Obstructive Urolithiasis | A brightly echogenic, highly reflective focal mass that casts a distinct, dark acoustic shadow directly posterior to its location within the kidney, ureter, or bladder. | Identifies the exact mechanical obstruction that is trapping urine and acting as a secure biological reservoir for the infecting bacteria. |
Hydronephrosis | Abnormal, pronounced dilation of the renal pelvis and internal calyces, appearing on the monitor as an interconnected network of dark, fluid filled spaces. | Confirms that a downstream physical blockage is actively forcing infected urine backward into the delicate filtering structures of the kidney. |
Accurately identifying these specific pathological markers, the radiologist transforms a vague clinical presentation into an exact structural diagnosis. This high resolution visual data allows the medical team to immediately differentiate between a simple mucosal inflammation and a severe, organ threatening complication.
Why Choose Koshikaa and Understanding the Clinical Report
When the diagnostic evaluation concludes, the radiologist generates a comprehensive urinary tract infection ultrasound report.
This highly detailed clinical document provides the referring physician with the exact quantitative measurements of the retroperitoneal organs and explicitly notes any structural abnormalities detected during the scan. The urologist relies heavily on these specific data points to formulate a highly targeted, definitive treatment strategy.
The clinical report typically highlights exact anatomical metrics, such as the specific millimeter thickness of the mucosal bladder wall or the precise cubic centimeter volume of retained urine. If the sonographic data indicates significant chronic urinary retention, the urologist may prescribe specialized alpha blocker medications to actively relax the bladder sphincter and improve fluid outflow.
‘Conversely, if the scan definitively identifies an obstructing renal calculus or a localized tissue abscess, the physician will immediately transition the patient from simple oral antibiotic therapy to a targeted surgical intervention to physically resolve the underlying pathology.
Conclusion
While routine bacterial infections of the lower urinary tract are highly common, recurrent or complicated clinical presentations demand immediate structural investigation.
Utilizing an advanced ultrasound for uti ensures that hidden anatomical defects, obstructive mineral stones, and severe inflammatory complications are accurately identified before they can cause irreversible ischemic damage to the renal tissue.
As this specific diagnostic modality utilizes safe acoustic waves rather than ionizing radiation, it remains the absolute gold standard for evaluating the urinary health of highly vulnerable populations, particularly pediatric patients and pregnant women.
Koshikaa operates as a premier diagnostic facility fully equipped to provide these critical retroperitoneal imaging services. Our highly trained clinical sonographers utilize state of the art acoustic technology to deliver flawless, high resolution diagnostic data directly to your referring physician. Do not ignore severe pelvic pain or recurrent urinary symptoms. Protect your long term renal health by ensuring an accurate, evidence based diagnosis.
Contact Koshikaa today to schedule your comprehensive urinary tract evaluation.