Managing irregular menstrual cycles, unexplained weight shifts, or persistent adult acne can feel deeply frustrating when you lack clear answers about your body’s internal health. Utilizing a targeted polycystic ovary syndrome (PCOS) ultrasound provides a non-invasive view of your internal anatomy, turning vague, distressing symptoms into clear, actionable diagnostic data.
Booking an advanced pelvic evaluation at a dedicated Health screening centre in Bangalore gives you the precise structural insights required to map your hormonal profile accurately and begin a targeted wellness strategy.
Hormonal and endocrine imbalances are rarely simple, isolated issues; they are complex metabolic conditions that affect your entire systemic well-being.
While experiencing a sudden shift in your physical health can feel overwhelming, understanding the structural and biological markers within your reproductive system brings immediate clarity.
We at Koshikaa believe that data-driven insights are the foundation of preventive wellness. By looking past surface-level symptoms to evaluate your internal baseline, we empower you to move away from guesswork and step confidently toward long-term lifestyle balance and vibrant health.
Medical Disclaimer
The diagnostic insights and educational concepts shared in this article are meant solely for informational purposes and do not substitute for professional medical advice, official diagnosis, or clinical treatment. Ovarian dynamics and hormonal structures vary significantly based on genetics, lifestyle, and age. Always consult a qualified gynecologist or healthcare professional to review your personal medical symptoms before modifying your health routine or initiating any therapeutic plan. Do not ignore or delay professional medical consultations based on the contents of this guide.
Diagnostic Gaps: Can Pelvic Imaging Confirm PCOS Independently?
A very frequent point of confusion when exploring Polycystic Ovary Syndrome (PCOS) and hormonal health is whether a single imaging session can provide a definitive diagnosis. It is incredibly common for someone to receive an ultrasound report showing a specific ovarian pattern and immediately assume they have PCOS. However, an ultrasound alone cannot confirm the condition. Looking at an image of the ovaries captures only one piece of a much larger metabolic and hormonal puzzle.
To provide an accurate answer: no, pelvic imaging cannot confirm this condition completely on its own.
The Medical Standard and The Rotterdam Framework

To avoid over-diagnosis and ensure clinical accuracy, medical professionals worldwide rely on an updated framework known as the Rotterdam Criteria. This standard establishes that a woman must meet at least two out of three distinct health markers to receive a formal diagnosis.
The three diagnostic pillars include:
- Ovulatory Dysfunction: This manifests physically as highly irregular periods, cycles that arrive more than 35 days apart, or the complete absence of a monthly cycle (anovulation).
- Androgen Excess: This involves elevated levels of masculine hormones, which can be identified physically through clinical signs like male-pattern hair thinning, severe cystic acne, and hirsutism (excess facial or body hair), or confirmed biologically via specialized blood tests that measure free testosterone.
- Polycystic Ovarian Morphology: This refers specifically to the structural layout of the ovaries as seen during visual imaging, showing a high concentration of tiny, resting follicles.
The Diagnostic Matrix of How Criteria Intersect
As this condition is a syndrome, meaning a collection of signs rather than a single disease, patients can present with vastly different combinations of these markers. The table below outlines how medical professionals evaluate these intersections:
| Patient Scenario | Clinical Symptoms | Imaging Findings | Diagnostic Outcome |
|---|---|---|---|
| Scenario A | Irregular cycles AND physical signs of high testosterone (acne/hirsutism). | Ovaries appear completely clear and typical. | Confirmed Diagnosis (Under international guidelines, imaging is not strictly required if the first two clinical signs are clearly present). |
| Scenario B | Perfectly regular, predictable menstrual cycles with no physical hair growth or acne. | The scan shows a high concentration of tiny fluid sacs. | No Diagnosis (An isolated visual finding in the absence of other hormonal symptoms does not meet the clinical threshold). |
| Scenario C | Highly irregular or missing periods, but normal hormone levels and clear skin. | Scan reveals an increased ovarian volume and high follicle count. | Confirmed Diagnosis (The combination of irregular cycles and structural imaging satisfies the two-out-of-three requirement). |
Why an Isolated Scan Falls Short
Relying entirely on a pelvic scan can create significant diagnostic gaps. Up to 25% of perfectly healthy women of reproductive age can display a polycystic appearance on an image without having the actual metabolic or endocrine syndrome.
This is especially true for young women within eight years of their first period, whose regular reproductive development naturally mimics this structural layout.
Brushing off symptoms or relying strictly on an individual scan can cause a delay in care. This is precisely why scheduling an ultrasound scan for PCOS is designed to act as a valuable structural map rather than an absolute, final answer. True health mapping requires looking at how these structural visuals connect with your daily metabolic health, fasting insulin levels, and complete lipid profiles.
Understanding that imaging is an investigative tool rather than a standalone judge, you can approach your screening session with total clarity, knowing that your visual data will be combined with biochemical markers to build a complete, accurate picture of your internal wellness.
Visual Anatomy of Identifying the Classic Physiological Markers

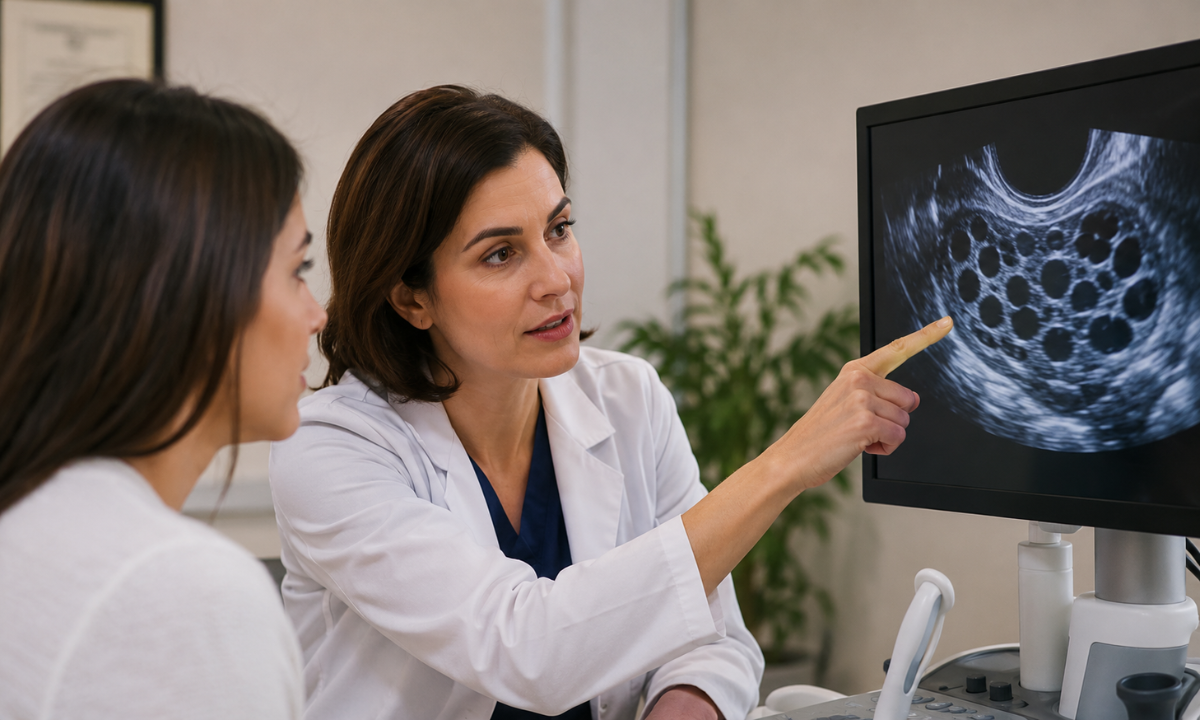
When you lie down for a pelvic imaging session, the sonologist is not just looking for a simple “yes” or “no” answer on the monitor.
They are actively measuring specific anatomical structures and mapping the precise micro-architecture of your pelvic organs. Understanding what the medical team tracks during this procedure helps demystify the entire process, turning a complex medical scan into a clear, logical evaluation of your reproductive health.
To get the most accurate look at the ovaries, specialists generally prefer a transvaginal ultrasound as it places the imaging probe closer to the pelvic organs, providing high-resolution details. If a transvaginal scan isn’t ideal or available, a transabdominal scan is performed across the lower abdomen with a full bladder acting as a clear viewing window.
The Radiologist’s Checklist for Key Structural Markers
During the scan, the specialist evaluates the size, shape, and internal patterns of the ovaries against specific guidelines to document key polycystic ovarian syndrome ultrasound findings:
- Follicle Count Per Ovary (FNPO): The specialist carefully counts the number of tiny, resting fluid sacs (antral follicles) visible in each ovary. Under current international diagnostic guidelines, seeing 20 or more of these small follicles measuring between 2 to 9 millimeters in either ovary points toward a characteristic pattern.
- Increased Ovarian Volume (OV): The system measures the three-dimensional size of the ovary to calculate its total volume. A typical, resting ovary is roughly the size of an almond. An ovarian volume greater than 10 milliliters in either ovary indicates enlargement, which frequently happens when a high number of resting follicles expand the structural tissue.
- The Peripheral Distribution Pattern: The specialist looks at where these tiny fluid sacs are located. In a classic presentation, the immature follicles gather tightly around the outer edges of the ovary, leaving the dense central tissue (the stroma) looking bright and solid on the screen.
It is important to understand that these numbers are highly specific baselines used by clinicians to ensure an accurate evaluation.
Finding an increased follicle count or a larger ovarian volume does not mean your health is failing; it simply means the natural cycle of follicle development has paused temporarily. By pinpointing these exact measurements, your clinical team gains the precise physical data needed to understand your unique endocrine profile and build a personalized care plan.
The Pathological Matrix: Decoupling Cysts from Follicular Arrays
Perhaps the single biggest source of unnecessary anxiety for women exploring this health profile is the word “cyst” itself. When a person hears that their ultrasound report mentions a cystic presentation, it is completely natural to imagine a dangerous, painful fluid mass that could grow, rupture, or eventually require surgical intervention.
This fear stems from a historical medical misnomer dating back to the 1930s.
In reality, the tiny, visible fluid structures captured during a scan are not true anatomical abnormalities at all. They are completely normal, healthy egg sacs (follicles) that simply paused in their natural growth cycle due to a temporary hormonal signal jam.
Clarifying the Ovarian Landscape
To understand exactly what is happening inside your pelvic architecture, it helps to compare how different fluid-filled structures behave. This distinction makes it clear why this specific polycystic ovarian pattern is completely distinct from standard pathological conditions:
| Ovarian Structure | Definition and Nature | Average Size Dimensions | Long-Term Lifecycle and Fate |
|---|---|---|---|
| Immature Antral Follicles (PCOS Profile) | Completely normal, healthy egg sacs containing undeveloped eggs that have paused their growth due to localized hormonal imbalances. | Exceptionally tiny, typically measuring between 2 mm to 9 mm in diameter. | They persist harmlessly inside the ovary for months, neither growing larger nor rupturing, until systemic metabolic balances improve. |
| Normal Dominant Follicle | A healthy, active fluid sac selected by the body during a standard monthly cycle to mature and release an egg. | Grows steadily throughout the month, reaching 18 mm to 24 mm right before ovulation. | Ruptures naturally mid-cycle to release a mature egg for potential fertilization, then dissolves away completely. |
| True Ovarian Cyst (Pathological/Functional) | A solitary, fluid-filled or solid sac that develops independently of the normal monthly egg-maturation cycle. | Considerably larger, frequently starting at 30 mm (3 cm) and sometimes growing up to several inches. | Can grow independently, occasionally causing localized pressure or discomfort, and may require medical monitoring or removal. |
The Science Behind the String of Pearls
During a standard, balanced menstrual cycle, your brain sends a wave of Follicle-Stimulating Hormone (FSH) to your ovaries at the start of the month. This signal recruits a small handful of resting follicles to begin growing. As the days pass, one clear leader emerges, becomes the dominant follicle, and the others naturally shrink away.
When your internal environment experiences subtle metabolic shifts, such as elevated fasting insulin levels, the communication lines become crowded. High insulin levels prompt the ovaries to produce slightly higher amounts of local androgens (masculine hormones). This subtle hormonal shift acts like a stop sign for the developing follicles.
Instead of one follicle growing to maturity and the others fading away, a dozen or more tiny follicles start the race but get stuck at the same early phase of development. As none of them can grow large enough to trigger ovulation, they remain visible on an ultrasound screen. They gather quietly around the outer edges of the ovarian wall, creating a circular, dark, pocketed layout that radiologists famously describe as a “string of pearls.”
Clinical Reality: These tiny fluid pockets do not cause physical pain, they do not tear the ovarian walls, and they do not require physical removal. They are simply highly visible indicators of a paused cellular cycle.
By looking at these visuals as a temporary biological pause rather than a permanent structural defect, you can remove the fear from your diagnostic journey and focus your energy on gentle, proactive lifestyle strategies that help reset your body’s natural operational rhythms.
Why Choose Koshikaa? Precision Preventive Diagnostics at Koshikaa
Navigating endocrine tracking requires advanced technology paired with deep clinical empathy. At Koshikaa, we move past isolated visual checkups to offer comprehensive health mapping that looks at your entire cellular and metabolic landscape. When you book an Ultrasound scan in Bangalore through our network, you choose a preventive experience tailored entirely around your comfort and long-term wellness.
Our screening environment stands out through these distinct clinical advantages:
- High-Fidelity Imaging Technology: We utilize premium diagnostic infrastructure to capture clear, detailed pelvic visuals, ensuring highly precise structural tracking.
- Empathetic, Women-Centric Care: Our clinical teams cultivate a warm, judgment-free space designed to minimize diagnostic anxiety during your visit.
- Integrated Metabolic Profiling: We combine your pelvic visuals with essential blood screenings to provide a complete picture of your metabolic health.
You receive clear, easy-to-read reports that translate complex clinical findings into practical steps for your lifestyle journey.
Conclusion
Uncovering a paused follicular cycle on an imaging monitor is not a roadblock; it is an empowering structural map of your body’s current state. Identifying these early physical markers gives you the precise information needed to step away from confusing symptoms and move toward proactive balance. By combining advanced, clear imaging with targeted metabolic tracking, you can confidently customize your lifestyle, reclaim your hormonal health, and build a vibrant, well-balanced life.