
Patients noticing a visible swelling in the anterior neck often seek immediate medical evaluation at a premier Health screening centre in Bangalore. This physical enlargement of the thyroid gland, clinically diagnosed as goiter disease, requires precise structural mapping to determine its underlying etiology.
When an endocrinologist or primary care physician observes this glandular hypertrophy, they typically order a high resolution Ultrasound scan in Bangalore to accurately evaluate the affected tissue.
The thyroid is a critical endocrine organ located at the base of the neck, responsible for producing hormones that strictly regulate systemic metabolism. When this tissue enlarges, the resulting structural changes can range from a benign, painless physical swelling to a massive, restrictive growth that severely compresses the adjacent trachea and esophagus.
As a simple physical examination cannot determine the internal composition or the functional status of the gland, a comprehensive diagnostic evaluation is strictly necessary. This clinical guide will provide a detailed overview of this endocrine condition by systematically addressing the following critical factors:
- The clinical identification of symptoms: We will outline the visible and mechanical signs of glandular enlargement, distinctly differentiating between minor cosmetic changes and acute airway compression.
- The underlying physiological triggers: We will examine the specific nutritional deficiencies and complex autoimmune dysfunctions that force the thyroid tissue to abnormally expand.
- The structural diagnostic protocols: We will detail how modern sonography maps the exact physical dimensions of the tissue and successfully identifies localized nodular growths.
- The established therapeutic interventions: We will review the precise medical, pharmacological, and surgical pathways utilized by physicians to restore normal endocrine function and resolve the physical swelling.
Understanding these fundamental diagnostic and therapeutic components, patients can actively participate in their endocrine care and recognize the absolute necessity of advanced radiological screening for any abnormal neck swelling.
Goiter Sign and Symptoms

The clinical presentation of an enlarged thyroid gland varies significantly depending on the overall size of the tissue, the rate of cellular growth, and the precise anatomical direction of the enlargement.
In early stages, a substantial number of patients remain entirely asymptomatic. However, as the glandular tissue expands beyond its normal physiological boundaries, it begins to physically interact with the densely packed vascular, respiratory, and digestive structures located within the anterior neck.
When patients present for a clinical evaluation, physicians systematically assess the structural and mechanical impact of the swelling.
The primary goiter sign and symptoms are directly related to the mass effect of the enlarged tissue pressing against adjacent anatomical pathways. The most frequently documented clinical manifestations include the following:
- Visible Anterior Neck Swelling: The most immediate clinical sign is a prominent, palpable lump at the base of the neck, which often becomes more visually apparent when the patient tilts their head back, shaves, or applies cosmetics.
- Globus Sensation: Patients frequently report a persistent, uncomfortable feeling of a foreign object or a tight constriction located deep within the throat, even when not actively swallowing.
- Dysphagia: As the posterior aspect of the thyroid gland enlarges, it directly compresses the adjacent esophagus, resulting in a documented difficulty or significant discomfort when swallowing solid foods or large pills.
- Dyspnea and Stridor: Substantial glandular growth can mechanically compress the flexible cartilage rings of the trachea. This physical obstruction causes severe shortness of breath or a high pitched wheezing sound known as stridor, which frequently worsens when the patient lies in a supine position.
- Vocal Cord Paresis: In advanced or highly invasive cases, the expanding tissue can compress the recurrent laryngeal nerve, causing sudden hoarseness, a scratchy throat, or a noticeable drop in the natural pitch of the patient’s voice.
The presence of any respiratory or swallowing difficulties strictly mandates an immediate structural evaluation to prevent acute airway obstruction.
Furthermore, if the glandular enlargement is driven by an underlying functional disorder, patients may simultaneously present with systemic metabolic symptoms. These secondary symptoms range from unexplained weight loss and resting tachycardia in hyperthyroid states to extreme fatigue and cold intolerance in hypothyroid states.
Carefully cataloging both the mechanical and systemic functional symptoms, the referring physician can determine the exact urgency of the required diagnostic imaging.
Primary Goiter Causes
The physiological mechanisms driving thyroid tissue hypertrophy are complex and directly relate to the biological synthesis of metabolic hormones.
The thyroid gland operates strictly on a negative feedback loop regulated by the pituitary gland. When this precise chemical signaling pathway is disrupted by nutritional deficits, cellular damage, or abnormal immune activity, the glandular tissue undergoes compensatory structural expansion.
Identifying the exact underlying trigger is the primary objective of the diagnostic evaluation.
When evaluating the primary goiter causes, endocrinologists classify the pathologies based on whether the resulting glandular enlargement is associated with hormone overproduction, hormone suppression, or normal metabolic function.
Dietary Nutritional Deficits
Historically and on a global epidemiological scale, the most prevalent form of goiter is caused by the deficiency of dietary iodine.
The human body cannot biologically synthesize iodine, meaning it must be absorbed entirely through diet. The thyroid follicular cells strictly require this trace mineral to manufacture thyroxine and triiodothyronine.
When systemic iodine levels drop critically low, the pituitary gland secretes massive volumes of Thyroid Stimulating Hormone to force the thyroid to capture any available trace iodine in the bloodstream. This chronic, unrelenting stimulation causes the entire organ to swell significantly.
Hashimoto’s Thyroiditis
In developed nations with adequate dietary iodine, this autoimmune disorder is the leading cause of glandular enlargement.
The patient’s own immune system erroneously produces destructive antibodies that attack and slowly degrade the healthy thyroid tissue. As the functional capacity of the gland drops, the resulting severe hypothyroidism forces the pituitary gland to continuously bombard the failing tissue with Thyroid Stimulating Hormone, leading to a firm, rubbery physical enlargement of the neck.
Graves’ Disease
This distinct autoimmune condition operates on the opposite end of the functional spectrum. The immune system generates a rogue protein known as Thyroid Stimulating Immunoglobulin.
This specific antibody perfectly mimics standard Thyroid Stimulating Hormone and permanently binds to the cellular receptors on the thyroid gland. This causes the tissue to continuously overproduce metabolic hormones, resulting in severe hyperthyroidism, while simultaneously forcing the gland to undergo massive, rapid physical expansion.
Physiological Hormonal Shifts
During pregnancy, the placenta naturally secretes Human Chorionic Gonadotropin.
As the molecular structure of this pregnancy hormone is remarkably similar to Thyroid Stimulating Hormone, it can mildly stimulate the maternal thyroid gland, leading to a temporary, benign diffuse enlargement that typically resolves postpartum.
Infectious Thyroiditis
A direct viral or bacterial infection of the upper respiratory tract can migrate into the thyroid tissue. This acute invasion triggers a severe inflammatory response, causing the gland to rapidly swell and become exceptionally painful to the touch.
To systematically categorize these diverse etiologies, clinical pathologists map the structural cause directly to its resulting functional metabolic state.
Diagnostic Correlation of Goiter Etiology and Functional Status
| Underlying Pathological Cause | Primary Physiological Mechanism | Resulting Systemic Thyroid Status |
| Severe Iodine Deficiency | Chronic overstimulation by the pituitary gland to maximize trace mineral absorption. | Initially Euthyroid (Normal), rapidly progressing to Hypothyroidism. |
| Hashimoto’s Thyroiditis | Autoimmune destruction of follicular cells leading to permanent synthetic failure. | Hypothyroidism (Underactive). |
| Graves’ Disease | Unregulated cellular stimulation by rogue immune system antibodies. | Overt Hyperthyroidism (Overactive). |
| Acute Viral Thyroiditis | Rapid tissue inflammation and the sudden release of pre synthesized stored hormones into the bloodstream. | Transient Hyperthyroidism, often followed by temporary Hypothyroidism. |
Utilizing comprehensive laboratory testing alongside advanced structural imaging, the referring physician can pinpoint exactly which of these biological mechanisms is driving the physical enlargement.
Understanding Goiter Multinodular
While the underlying physiological trigger dictates the metabolic hormone status of the patient, the physical architecture of the enlarged tissue directly determines the necessary medical or surgical intervention.
A clinical physical examination combined with high resolution sonography allows the endocrinologist to classify the macroscopic structure of the glandular hypertrophy into two primary diagnostic categories.
Understanding the exact cellular distribution of the enlarged tissue is strictly required to formulate an accurate long term prognosis and select the safest therapeutic pathway.
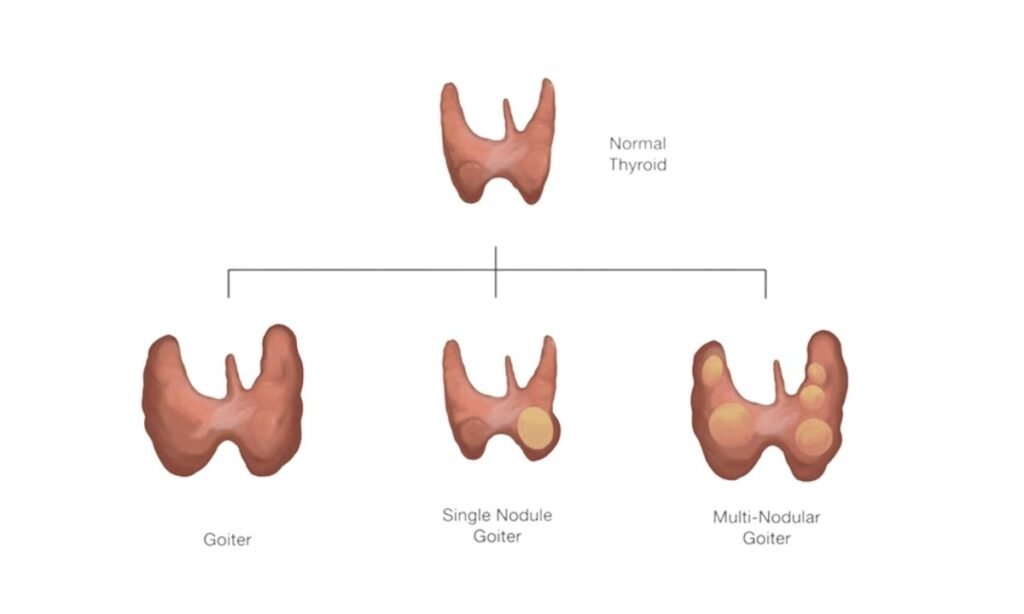
Diffuse Goiter
This structural classification occurs when the entire thyroid gland undergoes uniform, symmetrical hypertrophy.
The expanding tissue retains its natural, bilateral butterfly shape but significantly increases in total volume. The surface of the gland remains smooth to the touch.
This uniform growth pattern indicates that every follicular cell within the organ is responding identically to the underlying physiological stimulus, which is most commonly seen in early stage iodine deficiency or active Graves’ disease.
Goiter Multinodular
A goiter multinodular presentation is defined by the highly irregular, asymmetrical expansion of the glandular tissue. Instead of a smooth surface, the thyroid develops multiple, discrete structural growths known as nodules.
These nodules can be solid masses of dense cellular tissue, or they can be cystic structures filled with fluid and necrotic cellular debris. This complex architectural presentation typically develops over several years or decades as the thyroid tissue undergoes repeated cycles of active stimulation followed by periods of cellular involution and scarring.
When a radiologist identifies a multinodular structure, they must immediately assess the independent functional status of the individual nodules. This specific pathology frequently transitions into a highly dangerous metabolic state.
Functional Classifications of Nodular Pathology
Non Toxic Multinodular Goiter: In this clinical state, the multiple physical nodules are strictly structural. The localized masses do not independently synthesize metabolic hormones.
The patient remains euthyroid, meaning their systemic hormone levels are completely normal. The primary medical concern in this state is strictly mechanical, focusing entirely on preventing the growing nodules from compressing the adjacent trachea or esophagus.
Toxic Multinodular Goiter: Over time, one or more of the structural nodules may biologically mutate and become completely autonomous.
These specific hyperactive nodules disconnect from the pituitary gland’s regulatory feedback loop and continuously pump massive volumes of thyroxine and triiodothyronine into the systemic circulation.
This results in severe, uncontrolled hyperthyroidism, requiring immediate pharmacological intervention or targeted radioactive ablation to destroy the rogue tissue.
Precisely mapping the physical structure of the gland, the medical team can prioritize the diagnostic evaluation of the most suspicious or functionally active nodules within the overall enlargement.
The Role of Sonography
When an endocrinologist detects a physical enlargement of the anterior neck, an immediate structural evaluation is medically necessary.
While a manual physical examination confirms the presence of a goiter, it cannot determine the internal tissue composition or accurately measure the exact dimensions of the gland. High resolution sonography serves as the primary, non-invasive diagnostic modality for mapping the exact architecture of the thyroid tissue.
During the examination, the clinical sonographer systematically evaluates the entire cervical region. The radiologist analyzes the resulting acoustic data to document several critical structural parameters:
- Total Glandular Volume: The sonographer captures precise measurements of the right lobe, left lobe, and the connecting isthmus to quantify the exact severity of the hypertrophy.
- Tissue Echogenicity: This refers to the acoustic brightness of the tissue on the monitor, which helps the radiologist differentiate between healthy cellular structures and areas of chronic autoimmune inflammation.
- Nodule Composition: The scan provides strict differentiation between solid cellular masses, which may require further pathological evaluation, and entirely benign fluid filled cysts.
- Internal Vascularity: The technologist applies specialized Doppler imaging to measure blood flow velocity within the gland. Vascularity significantly increases in active Graves’ disease or within aggressive, hyperactive nodular growths.
- Cervical Lymph Nodes: The evaluation includes a comprehensive scan of the adjacent lymphatic structures to rule out localized abnormal lymph node enlargement.
To standardize the reporting of these specific findings, radiologists strictly analyze the physical characteristics of any identified nodules.
The acoustic data directly dictates the immediate clinical pathway, ensuring that dangerous pathologies are rapidly biopsied while benign growths are safely monitored.
Diagnostic Mapping of Nodular Characteristics
| Sonographic Feature | Benign Clinical Presentation | Suspicious Presentation (Requires Biopsy) |
| Internal Composition | Purely cystic (fluid filled) or spongiform architecture. | Solid cellular tissue or predominantly solid mass. |
| Margins and Borders | Smooth, well defined, and completely encapsulated. | Irregular, lobulated, or clearly extending into adjacent healthy tissue. |
| Acoustic Calcifications | Large, coarse macrocalcifications or a continuous calcified rim. | Microcalcifications appear as tiny, bright punctate echoes within the tissue. |
| Shape and Orientation | Wider than it is tall when viewed on a transverse imaging plane. | Taller than it is wide, indicating aggressive and abnormal cellular division. |
Patients frequently inquire about the financial aspect of this critical diagnostic step prior to scheduling their appointment.
The standard thyroid scanning price depends on the specific diagnostic facility and the required depth of the evaluation, including whether advanced Doppler vascular mapping is medically necessary.
Koshikaa maintains strict financial transparency, ensuring that patients receive elite, high resolution endocrine imaging at accessible diagnostic rates. This commitment allows referring physicians to obtain the exact structural data required to formulate an effective treatment plan without causing undue financial hesitation for the patient.
Why Choose Koshikaa? Comprehensive Goiter Treatment
Once the diagnostic imaging and laboratory tests identify the specific structural and functional pathology, the endocrinologist will formulate a targeted intervention plan.
The primary objectives of comprehensive goiter treatment are to restore normal systemic metabolic function, relieve any mechanical compression on the anterior neck structures, and completely eradicate any malignant or highly suspicious cellular growths.
As thyroid enlargement stems from diverse physiological triggers, there is no single universal remedy. The medical team selects the safest therapeutic pathway based entirely on the patient’s current hormone levels and the physical architecture of the gland mapped during the ultrasound.
Primary Therapeutic Pathways for Thyroid Enlargement
Active Clinical Observation
If the high resolution sonogram confirms that the goiter is small, completely benign, and causing no compressive symptoms, the physician may simply choose watchful waiting.
The patient will undergo routine annual thyroid scans and blood tests to strictly monitor for any future structural changes or functional shifts.
Pharmacological Hormone Regulation
For patients diagnosed with an underlying functional disorder, daily oral medications are the first line of defense. If the goiter is driven by Hashimoto’s thyroiditis and severe hypothyroidism, the physician prescribes synthetic levothyroxine to replace the missing hormones and suppress further pituitary stimulation.
Conversely, if the enlargement is fueled by Graves’ disease, antithyroid medications such as methimazole are utilized to actively block the synthesis of excess thyroxine.
Radioactive Iodine Therapy
This non surgical ablation technique is highly effective for treating a toxic multinodular goiter or severe hyperthyroidism. The patient ingests a carefully calculated dose of Iodine-131.
The hyperactive thyroid cells rapidly absorb this radioactive isotope, which then destroys the overactive tissue from the inside out. This precisely targeted radiation permanently shrinks the total volume of the goiter and resolves the toxic hormone overproduction.
Surgical Thyroidectomy
Total or partial surgical removal of the thyroid gland is the definitive clinical intervention for massive, obstructive goiters that restrict breathing or swallowing.
Furthermore, surgical resection is absolutely mandatory if the diagnostic ultrasound and subsequent fine needle aspiration biopsy confirm the presence of malignant cancer cells within a structural nodule.
Targeted Clinical Scenarios and Expected Outcomes
| Diagnostic Pathology | Standard Clinical Intervention | Primary Therapeutic Objective |
| Benign Euthyroid Goiter (Small) | Annual clinical and sonographic monitoring. | To prevent unnecessary medical intervention while ensuring the tissue remains stable. |
| Hypothyroid Diffuse Goiter | Daily levothyroxine replacement therapy. | To normalize systemic metabolism and halt further Thyroid Stimulating Hormone driven growth. |
| Toxic Multinodular Goiter | Radioactive Iodine (I-131) ablation. | To destroy autonomous hyperactive nodules and physically shrink the glandular volume. |
| Massive Obstructive Goiter | Total or near total surgical thyroidectomy. | To provide immediate mechanical relief for the compressed trachea and esophagus. |
Carefully aligning the structural acoustic data with the biochemical laboratory results, the medical team ensures that every patient receives the most appropriate and effective intervention for their specific endocrine condition.
Conclusion
Identifying a visible swelling in the anterior neck is the critical first step in managing goiter disease. As this structural enlargement can stem from nutritional deficiencies, autoimmune disorders, or complex nodular growths, a highly accurate diagnostic evaluation is strictly necessary.
After combining comprehensive laboratory testing with advanced structural sonography, physicians can pinpoint the exact physiological trigger and implement the most effective medical or surgical goiter treatment.
Koshikaa stands as a premier diagnostic facility dedicated to providing these essential endocrine imaging services. Our state of the art ultrasound technology delivers the high resolution structural data your physician requires to formulate a precise, personalized clinical pathway. Do not delay the evaluation of an enlarged thyroid gland.
Contact Koshikaa today to schedule your comprehensive diagnostic scan and protect your long term metabolic health.